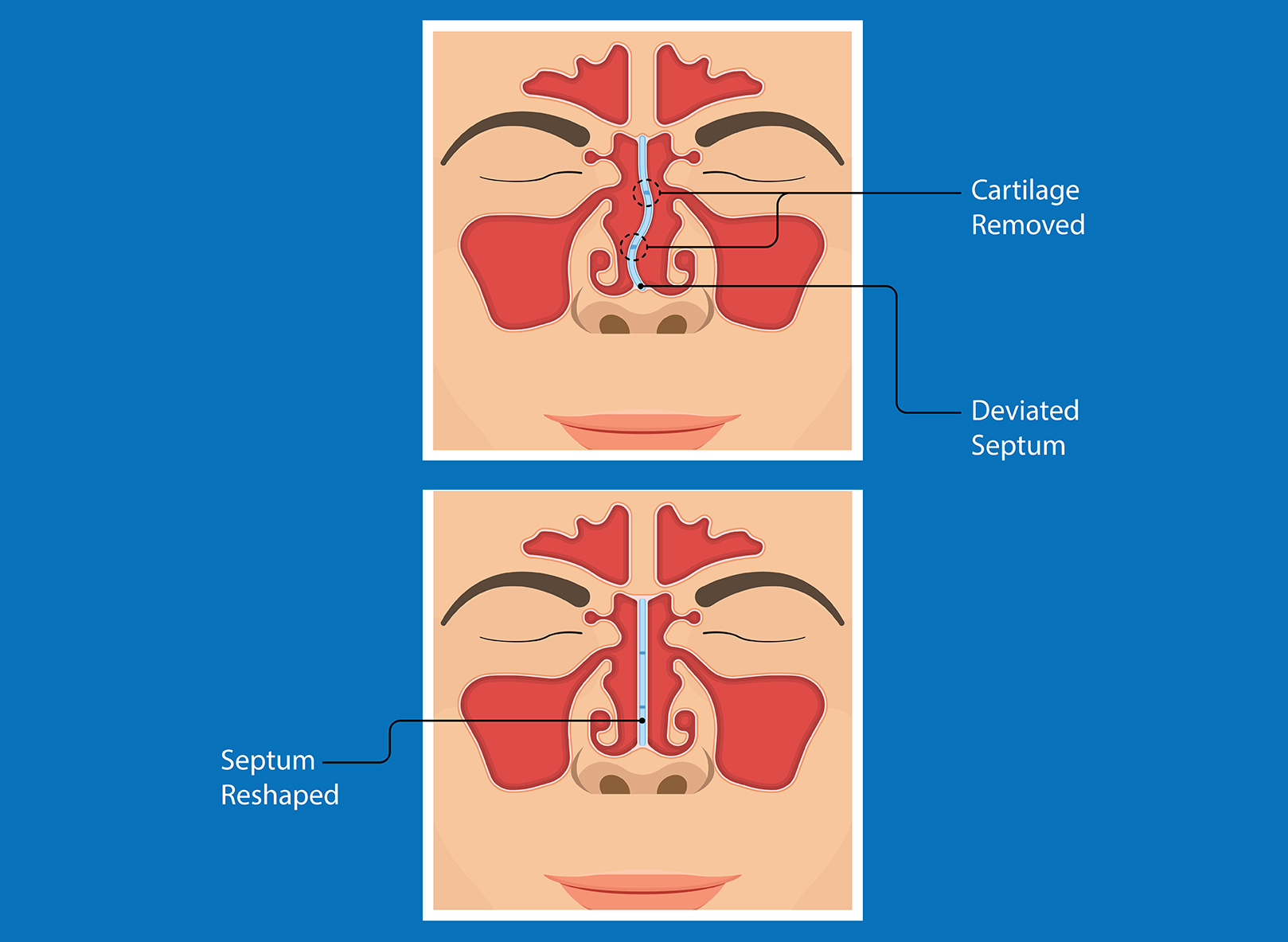
The nasal septum, comprised of cartilage and three separate bones, divides one nostril from the other. In many people, the septum becomes crooked as they grow and these bones begin to ossify, or harden. In some cases, nasal trauma may cause a fracture that distorts the septum. The result may cause significant blockage of airflow through one or both nostrils. For patients with chronic nasal congestion who do not respond to appropriate medications such as oral antihistamines, leukotriene antagonists, nasal steroid and antihistamine sprays, and even allergy immunotherapy, septoplasty may be necessary to improve nasal airflow.
Dr. Karanfilov performs septoplasty under general anesthesia in the OR. An incision is made inside the nose, and the mucous membranes are lifted off the septal cartilage and bone on both sides. Instruments are then used to remove deviated portions of cartilage and bone until the septum can assume a midline position. The mucous membranes are then sewn back together is mattress, or quilting, fashion to prevent blood from accumulating in the space where the cartilage and bone used to be. Dr. Karanfilov then inserts flexible plastic polymer splints along each side of the septum, since in his experience these increase the likelihood that the septum will remain in the midline. Dr. Karanfilov then sees his patients one week after surgery to remove the splints.